All published articles of this journal are available on ScienceDirect.

Transmission and Transmissibility of SARS-CoV-2: What We Know and What We Not
Abstract
Declared as a pandemic on March 11, 2020, COVID -19 has made it essential for the entire world to control and ensure safety measures for such infections in the future. To take any measures, one must be sure of the route of transmission of the agent causing Pandemic. With so many controversies in its mode of spread, COVID-19 has raised questions for the researchers to confirm its various modes of spread. Many of these modes can be overlooked; it is necessary to emphasize and illustrate them. The aim of this paper is to provide a brief overview of the various modes of COVID-19 transmission. According to the published literature, COVID-19 is primarily transmitted from person to person through oral and respiratory aerosols, with droplets from the virus-infected environment playing a minor role in disease transmission. The infection is particularly dangerous for healthcare workers and the elderly with comorbidities.
1. INTRODUCTION
Respiratory tract infections caused by viruses have now emerged as a leading cause of death and morbidity worldwide [1], with COVID-19 taking a huge toll of human life and representing an enormous economic and disease burden. SARS-CoV-2 and the associated coronavirus disease 2019 (COVID-19) pandemic have been shown to be transmitted through respiratory droplets and direct contact with an infected person [2], but its transmissibility through airborne transmission or indirect contact via contaminated inanimate surfaces is still debated [3].
Scientific experts believe that SARS-CoV-2 is an airborne virus that can be spread by viral aerosols [4]. Infectious viral aerosols will hang around in the air for a long time. SARS-CoV-2 can live for up to 16 hours in the air, according to reports, which is why continuous successful air purification is recommended. Dining areas, common areas, waiting rooms, offices, restrooms, and elevators all pose a major risk of airborne transmission.
Droplets are larger (>5µm) entities that fall to the ground rapidly due to gravity, typically within 3 to 6 feet of the source entity. Aerosols are tiny particles less than 5µm that evaporate quickly and leave behind droplet nuclei, which are tiny and light enough to float in the air for hours. similar to pollen [5].
1.1. Why Mode of Transmission Matters
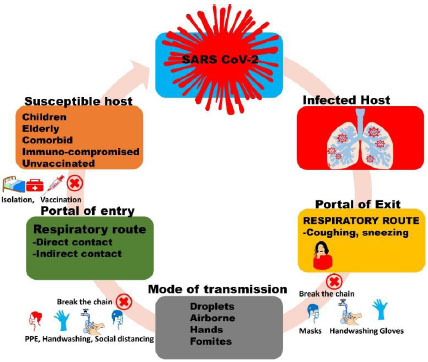
Broadly talking about all respiratory viruses, they can be spread in three ways:
a) Contact Transmission: Infection is transmitted by direct interaction with an infected individual e.g., handshaking or direct touching or through contact with a contaminated object or surface [6]. Fomite transmission is a term used to describe the above.
b) Airborne transmission is an infection transmitted by inhaling respiratory droplets containing viruses, made up of smaller droplets and particles that can float in the air for long time periods and distances usually more than 6 feet. They last in the air for a nearly infinite period [1].
c) Droplet transmission is by respiratory droplet containing virus i.e., larger and smaller droplets and particles exhaled by an infected person leading to spread in infection. When anyone is near to an infected individual, normally within 6 feet, transmission is most probable. They just stay in the air for 17 minutes [7].
The preliminary recognition of various modes of transmission of COVID-19 could be used to improve intervention strategies and subsequently their spread preventing and controlling epidemics and pandemics of similar viruses in the future [6].
We present a summary of the available evidence from various studies on COVID-19 transmission routes among individuals, identify knowledge discrepancies and discuss how the available knowledge can be used to apply control measures of this infection.
2. METHODS
Various Google searches were done in the months of February and March 2021 for manuscripts on various COVID-19 and other Coronaviruses' modes of transmission like SARS and MERS. Various sites that were used for searching articles were WHO, PubMed, CDC and Google Scholar. The different types of keywords that were used in searches were COVID-19 transmission, routes, airborne, control measures and their combination.
2.1. Eligibility and Data Screening
The final articles included in the study fulfilled the following criteria:
1) Articles Stating Laboratory Confirmed Modes of transmission of COVID-19
2) Articles with full text and peer-reviewed
Routes of transmission were assessed based on data obtained from various papers. Since the data was derived from publicly accessible databases and patients were not directly involved, this research did not require ethical approval.
3. RESULTS AND DISCUSSION
More than a year ago, In Wuhan, China, a SARS-CoV-2 outbreak occurred, which slowly spread far and wide and erupted in the form of a pandemic. Based on the two different statements by CDC on its website, earlier mentioning the airborne transmission of COVID-19 and later withdrawing the same [8], a lot of controversies are there on the modes of transmission of this virus. Respiratory viruses can be transmitted through three different routes: direct or indirect touch, droplet transmission, and aerosol transmission [1]. Although being a Respiratory Virus, COVID-19 is suspected of having Faeco-oral [9] and Mother to child [10] transmission. Table 1 summarizes various studies indicating the different modes of transmission of COVID-19.
It's crucial to figure out if droplets or aerosols play a bigger role in SARS-CoV-2 transmission as type of precautions vary for the two modes [21]. Wearing a surgical mask, face shield, or standing at least 6 feet away from other people should be enough to prevent transmission if COVID-19 is primarily transmitted through respiratory droplets, contrary to which if the virus is spread by aerosols then it can remain in the environment for an extended period of time consequently wearing a surgical mask would be insufficient, face shields can only have limited defense and maintaining 6 feet distance would not protect you from the virus particles carried by air currents.
| Airborne and Fomite Transmission | |||
|---|---|---|---|
| Study Name | Finding | Place | Reference |
| Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China, 2020 | “Data indicated that indirect transmission of the causative virus occurred, perhaps resulting from virus contamination of common objects, virus aerosolization in a confined space, or spread from asymptomatic infected persons.” | China | [11] |
| Evidence for probable aerosol transmission of SARS-CoV-2 in a poorly ventilated restaurant | “Aerosol transmission of SARS-CoV-2 due to poor ventilation may explain the community spread of COVID-19.” | China | [12] |
| Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1 | “Aerosol and fomite transmission of SARS-CoV-2 is plausible since the virus can remain viable and infectious in aerosols for hours and on surfaces up to days.” | Hamilton, MT | [13] |
| Detection and infectivity potential of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) environmental contamination in isolation units and quarantine facilities | “Despite prolonged viability of SARS-CoV-2 in controlled conditions, aerosol or indirect transmission from inanimate surfaces around hospitalized or quarantined COVID-19 patients is not supported by the data presented in this study.” | Israel Institute for Biological Research | [2] |
| Airborne Transmission of SARS-CoV-2 Theoretical Considerations and Available Evidence | “It is impossible to conclude that aerosol-based transmission never occurs and it is perfectly understandable that many prefer to err on the side of caution, particularly in health care settings when caring for patients with suspected or confirmed COVID-19. However, the balance of currently available evidence suggests that long-range aerosol-based transmission is not the dominant mode of SARS-CoV-2 transmission.” |
Boston, Massachusetts | [14] |
| Aerosol transmission of SARS-CoV-2? Evidence, prevention and control | “Evidence to date, however, is ample to acknowledge and address the aerosol transmission of COVID-19 in healthcare settings, other workplaces, and in the community.” | China | [15] |
| Mother Child transmission | |||
| Analysis of SARS-CoV-2 vertical transmission during pregnancy | “The SARS-CoV-2 genome was detected in umbilical cord plasma, indicating that in utero mother-to-child transmission, although rare, is possible and apparently related to a high maternal and foetal inflammatory state.” | Milan, Italy | [16] |
| Vertical transmission of coronavirus disease 2019: a systematic review and meta-analysis | “Vertical transmission of severe acute respiratory syndrome coronavirus 2 is possible and seems to occur in a minority of cases of maternal coronavirus disease 2019 infection in the third trimester.” | New Haven, CT | [10] |
| Possible Vertical Transmission of SARS-CoV-2 From an Infected Mother to Her Newborn | “We report a newborn with elevated IgM antibodies to SARS-CoV-2 born to a mother with coronavirus disease 2019 [COVID-19].” | Hubei, China | [17] |
| Faeco-Oral transmission | |||
| Detection of Novel Coronavirus by RT-PCR in Stool Specimen from Asymptomatic Child, China | “Our the finding of multiple positive stool specimens in this case similarly raises the concern that stool from COVID-19 patients might serve as another vehicle for virus transmission.” |
Zhoushan, China | [18] |
| The first detection of SARS-CoV-2 RNA in the wastewater of Tehran, Iran |
“The high values detected in effluent wastewater from local wastewater treatment plants have several implications in health and ecology that should be further assessed.” | Tehran, Iran | [19] |
| Characteristics of pediatric SARS-CoV-2 infection and potential evidence for persistent fecal viral shedding | “We also observed positive real-time RT–PCR results in rectal swabs in eight out of ten pediatric patients, which remained detectable well after nasopharyngeal swabs turned negative, suggesting that the gastrointestinal tract may shed virus and fecal–oral transmission may be possible.” | Guangzhou, China | [20] |
Respiratory droplets and direct contact have been a well-established mode of transmission of COVID-19 [22]. Cai et al. have laid the importance of COVID-19 transmission by fomites (Indirect Spread) and aerosolization of virus in confined spaces [11]. Their findings also suggest the transmission by Restrooms and Elevators (Fomites) and through asymptomatic persons. Doremalen et al. studied SARS-CoV-2 stability on different surfaces and calculated viral decay rates [13] after comparing the virus stability on artificially generated aerosols and surfaces like plastics, copper, cupboard, stainless steel, they inferred that COVID-19 spread by aerosol or fomite is possible since the virus can survive for hours in aerosols and days on surfaces. Contrary to this, in a study from Israel, surface and air samples accounted for 46% of the total viral RNA contamination. However, no viable SARS-CoV-2 was isolated from any environmental sample, but that may have happened as the CT value of samples >34. Another study has also reported the presence of non-viable viruses above CT value 34 [23].
Li et al. [12] looked into a restaurant outbreak involving three separate families in China’s Guangzhou and concluded that though near contact and fomite exposure are thought to be important factors in SARS-CoV-2 propagation, the virus can also be spread through short-range aerosol transmission in crowded and suffocating enclosures. After an outbreak following a weekly rehearsal in Skagit Valley, Washington, Miller et al. conducted a case study using questionaries [24] and suspected the aerosols released while singing rehearsal as a primary mode of spread in this case as all other direct and contact precautions were observed. Tang et al in their review article, have emphasized the credible evidences of airborne transmission of COVID-19 and their plausibility metrics scored 8 out of 9 for the same [15].
Mother-to-child transmission is another major concern in the spread of COVID-19.in a metanalysis done by Kotlyar et al. [10]. They found that among 936 infants from COVID-19 positive mothers, 27 (3.2%) had a positive result and concluded that vertical COVID-19 transmission is possible. and it tends to happen in a small percentage of cases mainly when the mother is infected in the last trimester. The incidence of infection is comparable to that of other pathogens that cause congenital infections. Anti-SARS-CoV-2 IgM and IgG antibodies were found in umbilical cord blood and milk samples, according to Fenizia et al. [16], emphasizing the virus's potential for vertical transmission. Dong et al. reported a case of elevated IgM antibodies in a newborn borne to a COVID-19 positive mother [25]. As IgM does not cross placenta and takes 3-7 days to rise after infection, the infection must have transferred in utero, yet again directing towards the vertical transmission of the disease.
| Route of Transfer | Transferred by | Mode | Precaution Required |
|---|---|---|---|
| Self-transfer | Self | Mucous membranes are self-inoculated by dirty hands. | Handwashing, Standard Precautions |
| Direct Contact | Contact with person | The spread of a virus from one infected person to another. | Handwashing, Standard Precautions, Gloves, PPE |
| Indirect Contact | Contact with Object | Virus transmission via infected intermediate objects (fomites). | Handwashing, Standard Precautions, PPE |
| Airborne | |||
| Droplet | Particle Size > 5µm | Coughing, sneezing, or breathing of an infected individual directly inoculates a naive person. | Surgical mask in addition to standard precautions Patient isolated or cohorting of patients with same infection is practiced Negative pressure in Patient room not required |
| Aerosol | Particle Size < 5µm | Aerosols in the respirable size range are inhaled. Deposition in the lower airways, as well as the rest of the respiratory tract. |
N95 mask in addition to standard precautions Patient isolated or cohorting of patients with same infection is practiced negative pressure in Patient room required |
Faeco-oral transmission by COVID-19 is yet another topic to explore as positive PCR results from stool specimen suggest that stool or sewage may also act as a mode of spread. The presence of virus in stool specimens was discovered by Tang et al. [18] even after negative respiratory tract specimens of the same individual and suggested stool should be considered for routine diagnostic screening in addition to respiratory tract specimens. SARS-CoV-2 RNA was positive in 8 out of 10 treated wastewater samples in an Iranian analysis [19]. We suggest that further studies are required to ascertain the faeco-oral transmission of COVID-19 as mere RT-PCR positivity may not be essential for virus's dissemination. To validate this mode of transmission, the virus must be viable when isolated from stool and sewage samples.
CONCLUSION
Droplet and direct contact are proven modes of transmission of SARS CoV-2. COVID-19 spread is thought to be caused by airborne transmission, with ventilation playing a key role. The evidence for SARS-CoV-2 transmission through aerosols, especially in well-ventilated environments, appears to be inconclusive. People should avoid closed and less ventilated spaces lest the pandemics come to a stop or should take precautions for airborne transmission as there are no perfect experimental data that can be used to prove or disprove SARS-CoV-2 transmission by aerosols. Mother Child transmission of COVID-19 through meagre but is possible. Proving faeco-oral transmission of this virus requires vast studies involving the culture of live virus from faecal specimens.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.