All published articles of this journal are available on ScienceDirect.

A Survey on COVID-19 pandemic in Karnataka State, India
Authors Info & Affiliations
Abstract
Aim:
The present study is aimed to survey and provide a detailed analysis of the spreading of the coronavirus and the controlling methods adopted in the state of Karnataka during the first three months.
Background:
Coronavirus has spread rapidly worldwide at a faster rate through primary contact followed by secondary contact without any symptoms in the initial stages and later on leading to fatalities. The viral spread was from person-to-person through the phylum droplets produced when an infected person sneezed or coughed. The increasing number of infected cases had put pressure on scientists worldwide to find a cure for it. Hence, a detailed survey may help control the viral spread by proper precautions with medication.
Objective:
The present report is a detailed survey of the coronavirus in the Karnataka state. It also reveals the entry of the coronavirus and its effects in the Karnataka state. Different lockdowns, day-wise, reported cases and also death cases are surveyed, which are discussed by plotting the required graph. Some medications and their implementations have also been discussed in the report.
Materials and Methods:
The data of the first three months has been considered to study the cumulative positive and death cases reported from the official website of the Karnataka state government and has been tabulated in the required form. Three-dimensional bar graphs have been traced using this data and the complete data has been analysed thoroughly.
Results:
Initially, the complete analysis of the positive and death cases has been revealed, referring to the four lockdown phases with bar graphs. Then, it was found that the increase in the number of positive and death cases was due to the increase in viral spread. In fact, the result of the concept of implementing Janata Curfew before the lockdown system was successful due to a good response from the public. However, some of the vaccines and other medication survey results showed that most of the countries have gone through the initial phases of the disease and have been moving towards the secondary findings. Age-wise and gender-wise, the study report indicates a high death rate in patients aged above 60, which may be due to their less resistance power. Significantly less spread rate and nil death rate has been observed in children aged below ten years due to their high resistance power.
Conclusion:
This survey report highlights the increase in the number of positive patients and death cases during all four lockdown periods. Further, it is stated that strict disciplinary actions against the public are required to maintain social distancing, which will reduce the positive cases. Likewise, the breakdown of human activities has been found to be the essential aspect in the COVID-19 reduction. Similarly, it was found that some of the other preventive measures like sanitization, use of masks and avoiding the possible public interaction proved to be a good measure to reduce the new cases. In addition to this, some of the proper available medication certainly supports the same.
1. INTRODUCTION
The deadly virus, i.e., the novel coronavirus named COVID-19 is a viral disease that affects humans' respiratory system and was first reported in Wuhan city of China. It also affects other parts of the human body, especially of those individuals who have weak immunity. This virus has spread rapidly across the world and hence it has been declared as a Pandemic by WHO. High fever, cold and cough, and breathing problems are the common manifestations [1-3]. It is highly contagious and can spread from one person to another at an alarming rate. It can spread very fast through primary contact than secondary contact without any symptoms in the initial stages and later on leading to fatalities.
It is not an air-borne disease, but it can spread by transferring droplets from infected to non-infected persons [4]. Because of its rapid spreading, maintaining social distancing is the main criterion to stop the pandemic's rapid spreading. Recent records show that it affects human beings who have less immunity, like old aged people and children under the age of ten and more death cases are that of old aged persons [5, 6]. This coronavirus can spread from person-to-person through the phylum droplets produced when an infected person sneezes or coughs. A person can also get infected by touching a surface or object with the virus present on it [7, 8]. Due to their bulky nature, these viruses cannot travel long distances. It can only affect if tiny droplets exiting from an infected person enter a non-infected person standing close by [9, 10]. Its lifespan outside its host cell varies from a few hours to a few days, which depends on various conditions and temperatures. In the process of spreading, these viruses have undergone mutations several times [11, 12]. A person with the laboratory confirmation of COVID-19, irrespective of clinical signs and symptoms, is considered a confirmed case of COVID-19; this has caused high morbidity and mortality in almost every country of the world. Generally, in the first phase, the patient is asymptomatic, and illness will take its peak during the second phase leading to dissemination at later stages if not treated in time. In the third phase, the infection rate curve will start to drop until the patent becomes stable. The total infection rate depends on preventive measures and effective treatments. The number of infected cases had put pressure on scientists worldwide to find a cure for it [13, 14].
The present report is a detailed survey of the coronavirus in Karnataka. It also reveals the entry of the corona virus and its effects in the Karnataka state. Different lockdowns, day-wise reported cases and also death cases have been surveyed and they are discussed by plotting the required graph. Some medication and its implementation have also been discussed in the report.
2. EXPERIMENTAL SURVEY
2.1. Entry of Coronavirus in Karnataka State
Bangalore is the capital city of Karnataka state, where the first COVID-19 case was reported on 8th March. A self-quarantined, Whitefield-based IT employee who returned from abroad was confirmed to be affected by COVID-19 positive followed by his wife and children. In addition to this, many positive cases were progressively reported in the state. The government planned to reduce the spreading by ordering to stop public gatherings and maintain social distance. It is the only first and foremost method to implement in the public sector to break the chain of spreading virus hence, the government initially announced a three-week lockdown of all the essentials [15].
2.2. First Death Case in Karnataka State
The first death case due to the coronavirus in Karnataka state was reported in the Kalaburagi district on March 13, 2020. A 76-year-old person who had returned from abroad died due to COVID-19 and the State Health Minister announced it after confirmation. Moreover, this COVID-19 patient suffered from hypertension and asthma disease [16]. The moment when it was announced publically by the government, the whole state was under a lot of fear about the coronavirus. Many negative thoughts started to spread in the form of discussions in public. Thinking of the wellbeing of the society, the government considered this very seriously and planned different measures to control the viral spreading.
2.3. Lockdown in Karnataka
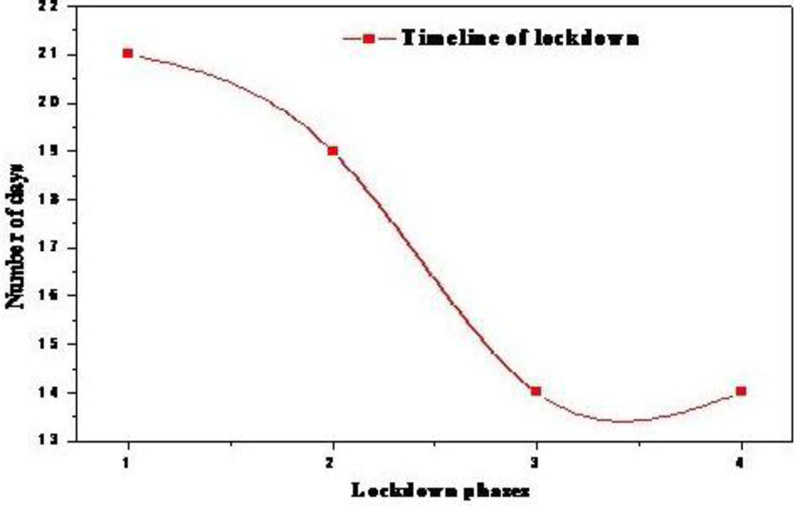
By March 2020, the corona virus had started spreading in our country, but before 12th March, there were no death cases reported. After a death due to COVID-19, the government considered implementing a serious lockdown for its control. Hence, four lockdown systems were implemented very strictly for 68 days (Fig. 1). Details of the lockdown phases are given in the Table 1.
2.4. First Lockdown
Immediately after the report of the first death case due to COVID-19 in Karnataka, the government announced a lockdown to maintain social distancing, which is one of the preventive measures of COVID-19. Under the Epidemic Diseases Act, the central government and the state government announced and implemented a lockdown strategy from March 25, 2020, to April 14, 2020, for 21 days and called this the first lockdown. This was implemented to avoid the spreading of the virus with multiple growths in human cells. Therefore, it was considered very seriously because of the non-availability of suitable medicines. In fact, the available medication in the market could neither control the viral spread nor treat the disease. Hence, the lockdown was the only implementing method on publics to stop the multiplication of the virus up to a considerable extent. Then, all the public activities in the state were completely suspended to maintain social distancing. Directives were issued to close all the public places with high footfall like malls, universities, colleges, cinema theatres, clubs, marriages, conferences, and mass gatherings, as a precautionary measure. All the state borders and district border transportations were completely shut down and sealed with curfew-like restrictions. The transports like KSRTC, BMTC, cab services, metro service, and national and international airway transportations were suspended to avoid mass gatherings. However, one of the essential services medical service was continued for the public, even when many cases were detected during the lockdown. After implementing preventive measures, the number of cases increased at a slower rate and was under control [17]. Some of the initially detected positive cases with details are given in Table 2. The slow growth rate of COVID-19 cases that was initially detected with travel history is also clearly revealed in Table 2.
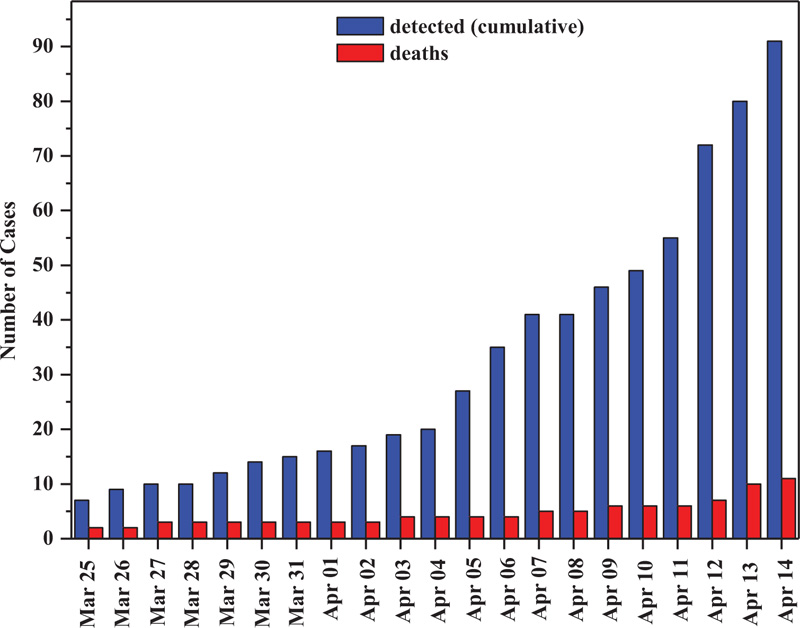
In addition to this, the number of cases detected and death cases during the first lockdown was surveyed thoroughly and the data is given in Table 3. The three-dimensional bar graph representing the detected cases and death cases during the first lockdown is shown in Fig. (2). This table clearly shows the cumulative increase in the detection of positive cases and an increase in the death cases along with the days. It also shows the slow spreading of the virus in the state with a cumulative increase in death cases. At the end of the first lockdown, a total of 91 new coronavirus cases and 11 death cases were detected within 21 days. This forced the government to take strict action against the virus control and implemented the second lockdown system to control the virus spread.
2.5. Second Lockdown
In connection with the increase in positive cases and death cases during the first lockdown, the government decided to implement the second lockdown with some more rigorous rules and regulations to control the virus in a better and more effective manner. Hence, the government announced a second lockdown from April 15, 2020, to May 3, 2020. Number of reported cumulative cases and death cases during second lock down are given in Table 4. An increase in the number of positive cases forced the government to extend the first lockdown period and it was called the second lockdown. During this lockdown period, the central government announced a fresh set of guidelines to be observed by all states and the same guidelines were implemented in Karnataka state (Fig. 3). Some of the essential strategies followed during that time are given below:
● All places of social gatherings, including religious conventions, were barred.
● Most of the Agricultural activities were exempted and allowed to be operated.
● All the Public work programs linked with the employment of daily-wage-labours with social-distancing measures were also exempted and allowed to be operated [18].
2.6. Third Lockdown
With the spike in viral cases, the government of Karnataka further extended lockdown till May 17 by following the central government direction. The government made three zones, namely, the red zone, orange zone, and green zone, following the number of cases detected in the specific places. Red zones were those with high coronavirus cases detected and a high doubling rate, orange zones were those with comparatively lesser cases, and green zones were those without any cases detected during the previous 21 days. The public movement on road transport was allowed in green zones with limited 50% capacity, i.e., single sitting arrangement with precautions. In orange zones, only private and hired vehicles were allowed, but public movement and other transportation were restricted (Fig. 4). The red zones remained under complete lockdown, similar to earlier stages [19]. Number of reported cumulative cases and death cases during second lock down are given in Table 5.
| S. No. | Phases | Lockdown Number | Period of Lockdown | No. of Days | |
|---|---|---|---|---|---|
| From | To | ||||
| 1 | Phase-1 | Lock Down-1 | 25 March 2020 | 14 April 2020 | 21 |
| 2 | Phase-2 | Lock Down-2 | 15 April 2020 | 03 May 2020 | 19 |
| 3 | Phase-3 | Lock Down-3 | 04 May 2020 | 17 May 2020 | 14 |
| 4 | Phase-4 | Lock Down-4 | 18 May 2020 | 31 May 2020 | 14 |
| Total lockdown days up to May 31, 2020 | 68 | ||||
| S. No. | Date | No of Cases Detected | Cumulative | Remarks |
|---|---|---|---|---|
| 1 | March 9 | 01 | 01 | IT Employs Returned from Abroad |
| 2 | March 10 | 03 | 04 | Wife and Children of the IT Employ |
| 3 | March 12 | 01 | 05 | The Old Man Returned from Abroad |
| 4 | March 13 | 01 | 06 | IT Employ |
| 5 | March 15 | 01 | 07 | - |
| 6 | March 16 | 03 | 10 | - |
| 7 | March 17 | 01 | 11 | - |
| 8 | March 19 | 01 | 12 | From Kodagu District |
| S. No. | Day |
No. of Detected Cases (Cumulative) |
No. of Death Cases |
|---|---|---|---|
| 1 | March 25 | 07 | 02 |
| 2 | March 26 | 09 | 02 |
| 3 | March 27 | 10 | 03 |
| 4 | March 28 | 10 | 03 |
| 5 | March 29 | 12 | 03 |
| 6 | March 30 | 14 | 03 |
| 7 | March 31 | 15 | 03 |
| 8 | April 01 | 16 | 03 |
| 9 | April 02 | 17 | 03 |
| 10 | April 03 | 19 | 04 |
| 11 | April 04 | 20 | 04 |
| 12 | April 05 | 27 | 04 |
| 13 | April 06 | 35 | 04 |
| 14 | April 07 | 41 | 05 |
| 15 | April 08 | 41 | 05 |
| 16 | April 09 | 46 | 06 |
| 17 | April 10 | 49 | 06 |
| 18 | April 11 | 55 | 06 |
| 19 | April 12 | 72 | 07 |
| 20 | April 13 | 80 | 10 |
| 21 | April 14 | 91 | 11 |
| S. No. | Day |
No. of Detected Cases (Cumulative) |
No. of Death Cases (Cumulative) |
|---|---|---|---|
| 1 | April 15 | 101 | 13 |
| 2 | April 16 | 107 | 14 |
| 3 | April 17 | 114 | 14 |
| 4 | April 18 | 126 | 14 |
| 5 | April 19 | 134 | 16 |
| 6 | April 20 | 136 | 17 |
| 7 | April 21 | 151 | 17 |
| 8 | April 22 | 166 | 18 |
| 9 | April 23 | 175 | 18 |
| 10 | April 24 | 192 | 18 |
| 11 | April 25 | 207 | 18 |
| 12 | April 26 | 216 | 20 |
| 13 | April 27 | 228 | 21 |
| 14 | April 28 | 241 | 22 |
| 15 | April 29 | 250 | 22 |
| 16 | April 30 | 269 | 23 |
| 17 | May 01 | 296 | 24 |
| 18 | May 02 | 315 | 25 |
| 19 | May 03 | 341 | 26 |
Table 5.
| S. No. | Day |
No. of Detected Cases (Cumulative) |
No. of Death Cases |
|---|---|---|---|
| 1 | May 04 | 361 | 27 |
| 2 | May 05 | 375 | 29 |
| 3 | May 06 | 403 | 29 |
| 4 | May 07 | 417 | 30 |
| 5 | May 08 | 427 | 30 |
| 6 | May 09 | 441 | 30 |
| 7 | May 10 | 486 | 31 |
| 8 | May 11 | 489 | 31 |
| 9 | May 12 | 502 | 32 |
| 10 | May 13 | 534 | 33 |
| 11 | May 14 | 556 | 35 |
| 12 | May 15 | 559 | 36 |
| 13 | May 16 | 619 | 36 |
| 14 | May 17 | 647 | 37 |
| Total | 14 days |
| S. No. | Day |
No. of Detected Cases (Cumulative) |
No. of Death Cases |
|---|---|---|---|
| 1 | May 18 | 694 | 37 |
| 2 | May 19 | 747 | 40 |
| 3 | May 20 | 795 | 41 |
| 4 | May 21 | 834 | 41 |
| 5 | May 22 | 910 | 41 |
| 6 | May 23 | 1050 | 42 |
| 7 | May 24 | 1182 | 42 |
| 8 | May 25 | 1296 | 44 |
| 9 | May 26 | 1414 | 44 |
| 10 | May 27 | 1525 | 47 |
| 11 | May 28 | 1655 | 47 |
| 12 | May 29 | 1925 | 48 |
| 13 | May 30 | 2075 | 49 |
| 14 | May 31 | 2538 | 51 |
| Total | 14 days | ||
2.7. Fourth Lockdown
On May 18, 2020, the chief minister of Karnataka announced the continuation of lockdown in the state up to May 31, 2020, with some relaxation after receiving the central government's guidelines. During this phase of the lockdown, most of the activities, excluding malls, theatres, and hotels, were permitted to operate between morning 7 and evening 7, except on Sundays. To restrict the activities on Sundays, the government had decided to implement a lockdown every Sunday, during this period the public activities were restricted [20]. The numbers of new cumulative cases detected and death cases have been tabulated in Table 6. The three-dimensional bar graph representing the detected cases and death cases during the third lockdown is shown in Fig. (5). This table and the figure show again a rapid increase in the positive virus cases along with an increase in death rate as well. During these 14 days, 2538 cumulative positive cases were recorded, with 51 death cases.
3. RESULTS AND DISCUSSION
3.1. Analysis of Lockdown System
The lockdown phases which were implemented in Karnataka are given in the Table 1 in the experimental section and the time tine graph of the lockdown system is represented in Fig. (1). The graphical figure represents the four lockdown phases with a number of days and represents the decrease in the number of days during the successive lockdown. Step-wise implementation of lockdown took place and also reduced the days, which may be due to the expectation of reduction of positive cases throughout the state. After implementing preventive measures, the number of cases increased at a slower rate and was under control [17]. During the first lockdown, initially detected positive cases with details have been given in Table 2 in the experimental section. The slow rate of COVID-19 cases was initially detected with travel history is vivid from Table 2. In addition to this, one can observe from the table that the first case was detected from IT employees who returned from abroad. The latter case also showed that again, an IT employee with his wife as well as his children. The increase of positive cases continued with an older adult who returned from abroad followed by again an IT employee and added to the cumulative number of positive cases. These results show that the viral infection started in the state from the people who returned from abroad. The number of new cases and death cases during the first lockdown has been tabulated in Table 3. The three-dimensional bar graph representing the detected cases and death cases during the first lockdown is shown in Fig. (2). This figure shows the cumulative increase in detection of positive cases and an increase in death cases along with the days. It also shows the slow spreading of the virus in the state with a cumulativeincrease in death cases. At the end of the first lockdown, a total of 91 new coronavirus cases and 11 death cases were detected within 21 days. This forced the government to take strict action against the virus control and hence implemented the secondlockdown system to control the virus spread.
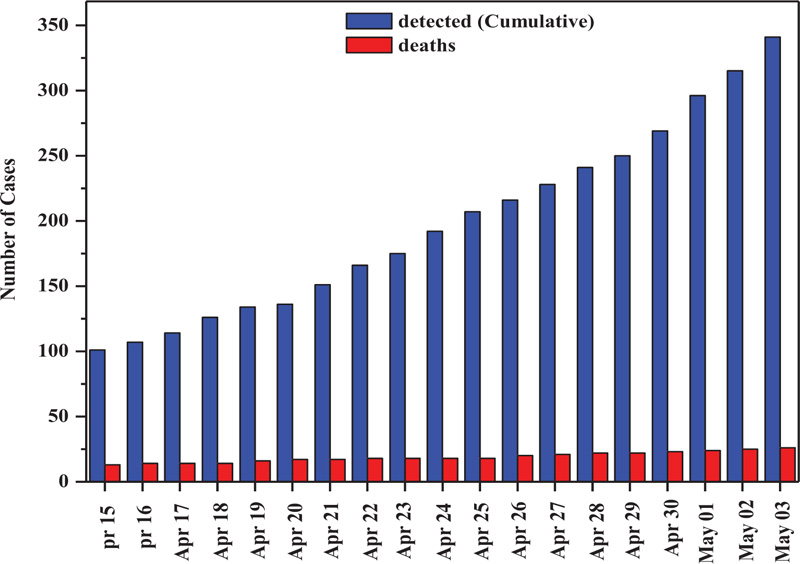
The number of cumulative cases detected with the number of death cases during the second lockdown period is given in Table 4 in the experimental section. The two-dimensional bar graph representing the detected cases and death cases during the second lockdown is shown in Fig. (3). These data reveal an increase in the number of new patients as well as death cases. During these 19 days of lockdown, 341 cumulative new patients and 26 cumulative death cases were detected. This data, when compared with the first lockdown data, confirms the progressive increase in detecting new positive cases and new death cases in the second lockdown as well. However, based on the guidelines issued by the central government, the chief minister of Karnataka announced the decision on relaxation on April 20th after evaluating the extent of public conformity to the lockdown [18].
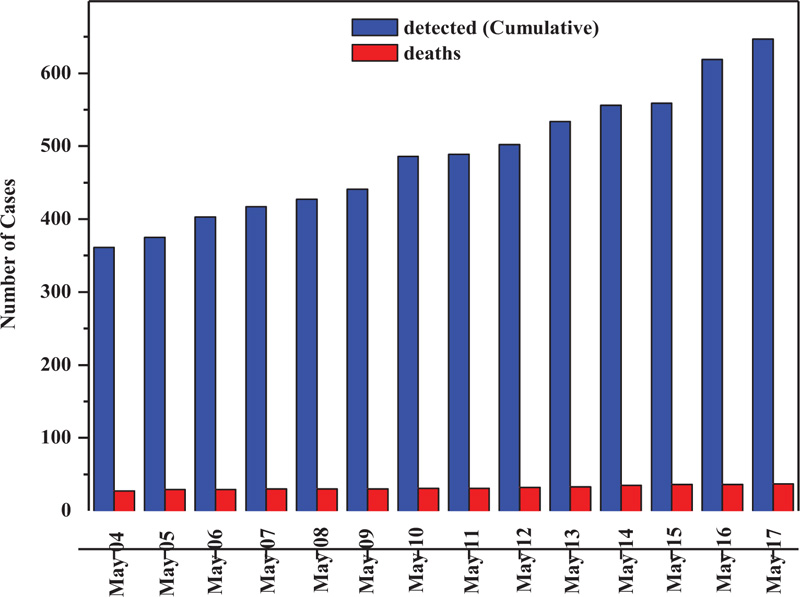
The positive cases and related deaths observed during this period and the data available are given in the Table 5 in the experimental section. The two-dimensional bar graph representations of detected cases and death cases during the third lockdown are shown in Fig. (4). Similar to the earlier lockdown, during this period also, the number of new cases and death cases was increasing. During these 14 days, a total of 647 cumulative new cases were detected, with cumulative 37 death cases. The zones classification was revised once a week [19].
The number of new cumulative cases detected and death cases are tabulated in Table 6 in the experimental section. The two-dimensional bar graph representations of the detected cases and the death cases during the third lockdown are shown in Fig. (5). This table and figure show again a rapid increase in the positive virus cases along with an increase in the death rate also. During these 14 days, 2538 cumulative positive cases were recorded, with 51 death cases [20].
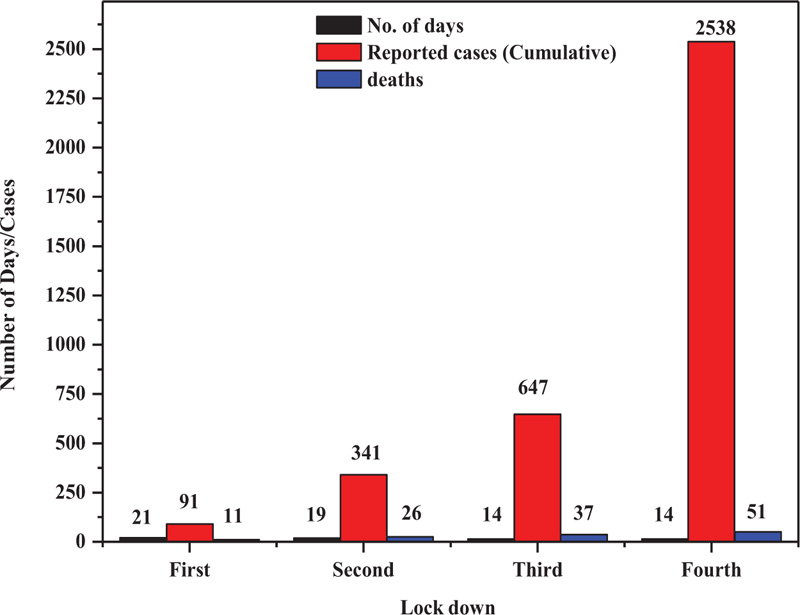
3.2. Comparative Study of Four Lockdowns
The comparative study of these four lockdown phases gives precise information about the variation in the reported cases and death cases. Table 7 shows the comparative reported cases and death cases in all four lockdown phases. Fig. (6) represents the two-dimensional bar graph of positive cases and death cases during this lockdown. It is observed from the table and figure that, during the first lockdown, the slow increase of the number of positive patients and prolonged increase of death cases, whereas in the second lockdown, progressive increase of the cases with a moderate increase of the death cases have been reported. Mutation of the virus took place even after the consideration of precautionary measures like social distancing and using the mask. During the first fourteen days of the third lockdown a further increase in the positive and death cases was observed. The death cases that crossed more than 37 hindered the implementation of strict disciplinary actions in controlling public activities. Multiplication of these controlling forces continued by the government and continued the lockdown system to reduce the number of multiple cases. But, during the fourth lockdown phase, the sudden increase in the new cases with an increase in death cases was observed. Moreover, these reports confused the public whether the virus spreads over community bases or it is still under control. Number of quarantines was increasing day by day; out of that some were under death cases and some were curable with available medication.
| S. No. | Lock Down | No. of Days |
Reported Cases (Cumulative) |
Death Cases (Cumulative) |
|---|---|---|---|---|
| 1 | First | 21 | 91 | 11 |
| 2 | Second | 19 | 341 | 26 |
| 3 | Third | 14 | 647 | 37 |
| 4 | Fourth | 14 | 2538 | 51 |

3.3. Janata Curfew in Karnataka
Soon after the first death case, and observing the virus spread in India, on March 22, 2020, Sunday, the Hon'ble Prime Minister, Sri. Narendra Modi ji requested the fellow citizens to maintain social distance by staying at home for an entire day and he called it as JANATA CURFEW. It was a self-imposed restriction for society's well-being and was the first action to fight against the coronavirus in our country. The Janata Curfew was made successful by the public, who with due respect to the prime minister's words, stayed indoors and exhibited their support to fight this virus [21].
3.4. COVID-19 Relief Funds in Karnataka
With the implementation of lockdown in the state to maintain social distancing, all financial activities were crippled and impacted the financial conditions of the state. Hence, the government of Karnataka called upon its citizens to financially contribute and lend a helping hand to fight against COVID-19 and called it as Chief Minister Relief Fund. The corporate sectors initially contributed Rs. 510 Million, Karnataka State Cricket Association (KSCA) contributed Rs. 5.1 Millions and BCCI contributed Rs. 5.1 Millions to the CM relief fund for fighting against the COVID-19 pandemic. Toyota Company added the same by distributing 1000 essential kits to daily wage workers, which benefitted over 5000 families, and distributed free-of-cost sanitizers and masks to the Police Department. The transportation department provided their buses to facilitate the state health department. The authority of Toyota Kirloskar Motor also donated Rs. 20 Millions to the state relief fund. Similarly, many donors (like government employees, NGO’s, politicians, etc.) donated to the state relief fund and they are noted for society's noble cause [22]. This kind of donation at the needy time helped the government to serve the needy people in a better way during this pandemic situation.
3.5. Medication
The whole world was in trouble due to the corona pandemic, and the countries all over the world were struggling a lot to find some medicine or vaccine at the earliest to help the lives on the earth. To date, no country has discovered suitable medicine to cure exactly this disease. Most of the countries have passed in preliminary results and have been moving towards secondary findings. Some countries like the US and Israel have cleared the second stage expecting good results. However, it was, almost inevitably, less successful in older people because of aged immune systems, which could not respond well to immunization. We can see this with the annual flu jab. In fact, the possibility to overcome this could be by either giving multiple doses or giving it alongside a chemical that gives the immune system a boost.
Following are some of the points which have to be carried out for the same.
● Many trials are required for safe medicine, and it must be free from side effects.
● Proper experimentation is needed for the medicine or vaccine to provoke an immune response, protecting people from getting sick.
● The success of the medication depends on trial experiments on humans.
● After the successful discovery of the medicine, it must be produced on a large scale to reach everyone.
● Its safety must be confirmed before its use.
● If a vaccine is developed, then there will be a limited supply initially, so it is important to prioritize.
Because of the overwhelming spread of the virus, the most powerful vaccine or medicines are required to break the chain from spreading infections. All over the globe, most scientists have involved themselves in the speedy discovery of effective drugs/vaccines, even though a vaccine fit for humans normally takes years to develop. Presently, many potential vaccines have passed the clinical stages and they have to pass the basic human trial version. Recently, the Italian government has claimed the successful discovery of antibodies for human cells. They also claim that the experimentation was thoroughly carried out and reported the proper neutralization in the body. Hence, these antibodies can block the effect of the virus in human cells. In addition to this, Oxford University has also announced a new vaccine called Elisa Granato which also passed the human trial. The vaccine - ChAdOx1 nCoV-19 developed by the University's Jenner Institute trials the final vaccine [23].
3.6. A Note On Plasma Therapy
It is a new technology developed for the treatment of COVID-19 patients. This therapy effectively treated the patients by transfusing a blood component from COVID-19 recovered patients. This kind of transfusion develops a passive immune system in the affected patients by producing several antibodies. These antibodies fight against the virus and reduce its effects. Karnataka is one of the states that took part in implementing this therapy for the treatment and showed the nearness in patients' recovery. It is not a medication process, but it shows the effective development in strengthening the human immune system of the human body to fight against viruses and it has been treated as an alternative treatment method. However, later there were some words against the therapy and that the highly infectious disease was at an experimental stage and could cause life-threatening transfusion-related complications [24].
3.7. A Note On Hydroxychloroquine Medicine
Hydroxychloroquine is a drug used to treat malaria, especially in India. In fact, it has been considered as a disease-modifying anti-rheumatic drug (DMARD) that is proved effective in regulating immune system function. Further, it has been considered as an antimalarial drug; however, it was found that it could not reduce the menace of malarial infection [25]. It also shows some effective medication properties like antiviral and immune development in the treatment of COVID-19. Some of the countries like the US have started the use of the same before confirming the clinical trials as it was the only available medication. Some of the initial trials reported that this medicine could be effective and competent enough to fight against the virus. Of course, it reduces common symptoms of a virus-like cold, fever, cough, etc. in the infected patients. However, this drug was not advised especially in India, thinking as prolonged usage of the same could result in poisoning [26]. Lately, a declaration from the National Institute of Health (NIH) endorsed against the use of hydroxychloroquine in the treatment of COVID-19 patients. Therefore, due to safety concerns and lack of efficacy, an emergency use authorisation for hydroxylcholoroquine was revoked for treatment of COVID-19 patients and the Diseases Society of America also supported it. Moreover, to add to the same, the guidelines panel for the treatment of COVID-19 patients endorsed against the usage of hydroxycholoroquine for the treatment of hospitalised and in non-hospitalised patients [27].
3.8. A Note on Remdesivir Drug
Remdesivir drug introduced by Gilead Sciences was also used to treat Ebola and the disease caused by the coronavirus family. It has also been shown to inhibit replication of other human coronaviruses associated with high morbidity in tissue cultures, including severe acute respiratory syndrome corona virus-like cold, coughs and fever. Hence, it may be considered as a medicine as well because it gives promising results by the speedy recovery of most symptomatic diseases and develops changes in the human body. In addition to this, the possible recovery rate improves in the affected patients. However, effective antiviral properties have been observed in the drug and hence it may be considered a drug for COVID-19. It is not recommended for those who are suffering from renal symptoms and in children. Further, it is also not advisable for the treatment in pregnant women [28-31]. Karnataka government has issued guidelines for the optimal usage of Remdesivir in the treatment of COVID patients in hospitals. However, it has also been said that Remdesivir's Emergency Use Authorization (EUA) may be considered only in the treatment of patients with moderate to severe disease (who require oxygen supply), and also the patient should have no renal or hepatic dysfunction. Similarly, it was suggested that it should not be used in the treatment of patients who require no oxygen support or they are in-home care settings.
During the second wave of COVID-19, the Department of Health and Family welfare officials had a meeting to discuss this proposal with the Association of Private Hospitals and Nursing Homes. During the meeting, the association members requested the officials that the supply of injection should be through the Karnataka State Drugs Logistics and Warehousing Society.
3.9. Age-Wise and Gender-Wise Split Of Total Cases
The COVID-19 spreading rate is in accordance with the age of the persons. As per the microbiologists, the spread rate is high in adults i.e., in the age group of 30-40 years and followed by the age group between 20-30 years due to high contact rate with others. Fig. (7) indicates the age-wise positive cases and Fig. (8) represents the gender-wise reported cases during the lockdown. The observation of Fig. (7) clearly shows that the reported male cases have been higher than female cases. The reason behind this may be the high exposure and contact rate of males with the public. The study of the reported cases indicates that the high death rate is in the aged persons who were above 60 years and maybe it was due to less resistance power. Significantly less spread rate and nil death rate in children i.e., aged below ten years, has been observed, which may be due to high resistance power.

3.10. COVID-19 Vaccination in Karnataka
Finally, the government of India launched two effective vaccines called Covaxin and Covisheld to fight against COVID-19. Presently, the government has not permitted the public to decide on their own as to which vaccine they have to get, however the result of the first phase clearly suggested that both the vaccines after being vaccinated in India were found to be safe and effective. The Bharat Biotech International Limited developed Covaxin in collaboration with the Indian Council of Medical Research (ICMR) and the National Institute of Virology (NIV). Oxford-AstraZeneca developed Covishield, and was manufactured by the Serum Institute of India (SIT). Lately, due to the spread of the highly effective Delta variant, the makers of both the vaccines started a new study in order to regulate the effectiveness of the third dose of covaxin to be considered as the booster dose. Covaxin has been developed with Whole-Virion Inactivated Vero cell-derived technology, whereas Covishield has been prepared using the viral vector platform technology. After usage, the result showed that the Covishield could be up to 90% effective and Covaxin could be 78-81% effective.
However, both the vaccines have been similar to vaccines made using inactive/modified versions of the virus. These vaccines worked as two-dose vaccines; they were administered weeks apart and injected intramuscularly [32, 33].
The government of Karnataka started vaccination very seriously as per the directions from the government of India to control the COVID-19 in the state. Therefore, district-wise planning was made with many camps to create awareness and educate the people about the effectiveness of the vaccines. After the success of the first dose vaccination, the second phase of COVID-19 vaccination in the state began. It has spread in two phases as of now. In the first phase, 4,09,836 healthcare workers and 86,798 frontline workers were administered the first dose of vaccine across the state with a coverage of 50 percent and 30 percent, respectively. The highest cumulative achievements of Health Care Workers (HCW) and Front-Line Workers (FLW) with 98,449 HCW and 11,683 FLW were administered the first dose of the COVID-19 vaccine. The lowest cumulative achievements of HCWs with 3,962 workers administered the first vaccination dose with the lowest FLWs achievements with only 762 workers. The second phase of the COVID-19 vaccination drive began from March 2021 for those who were above 60 years and those above 45 years with co-morbidities. In order to identify the beneficiaries, the Health Department of Karnataka started a door-to-door survey across the state. In fact, the state government has been showing tremendous progress in countering the menace of COVID-19. As of 29th September 2021, a total of 55940791 people had successfully received both the doses of vaccine in Karnataka state and they are considered to be fully vaccinated [34]. This kind of vaccination has been found to be of great help in controlling the spreading of the virus and finally to contain it completely.
CONCLUSION
This survey report, in conclusion, reveals the increase of the positive patients and death cases during all four lockdown periods. Further, strict disciplinary actions against the public are required to maintain social distancing, which reduces the rate of positivity. Break down in human activities is a very essential aspect of the COVID-19 reduction. Some of the other precautionary measurements like sanitization, use of masks and avoiding the possible public interaction may reduce the new cases and hence it will be under control. In addition to this, some of the proper available medication may also support the same.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The authors of this survey endorse that the data supporting the findings of this study are available in the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors thank the authorities of Vijayanagara Sri Krishnadevaraya University, Ballari for constant support and encouragement. Thanks are due to Prof. A. Venkataraman, Professor, Department of Chemistry, Gulbarga University, Kalaburagi, Karnataka, India for useful discussion in drafting the study material.

